
To supplement my post about borderline personality disorder (BPD), I’ll comment on a highly effective therapy developed especially for BPD. I, myself, have been through DBT and can attest to its wonderful results. DBT is a modified form of cognitive behavioral therapy (CBT). CBT focuses on addressing cognitive distortions (thoughts that assume negative reasons for a potentially neutral situation) and practicing changing the way you think about the situation. DBT focuses on accepting the way you think, but changing the way you react to the thoughts.
DBT was created by Marsha Linehan for patients with BPD, but is now used for many other disordered patients who suffer from suicidal ideation and self-harm. DBT teaches skills that a person can use to react healthily to difficult emotions.
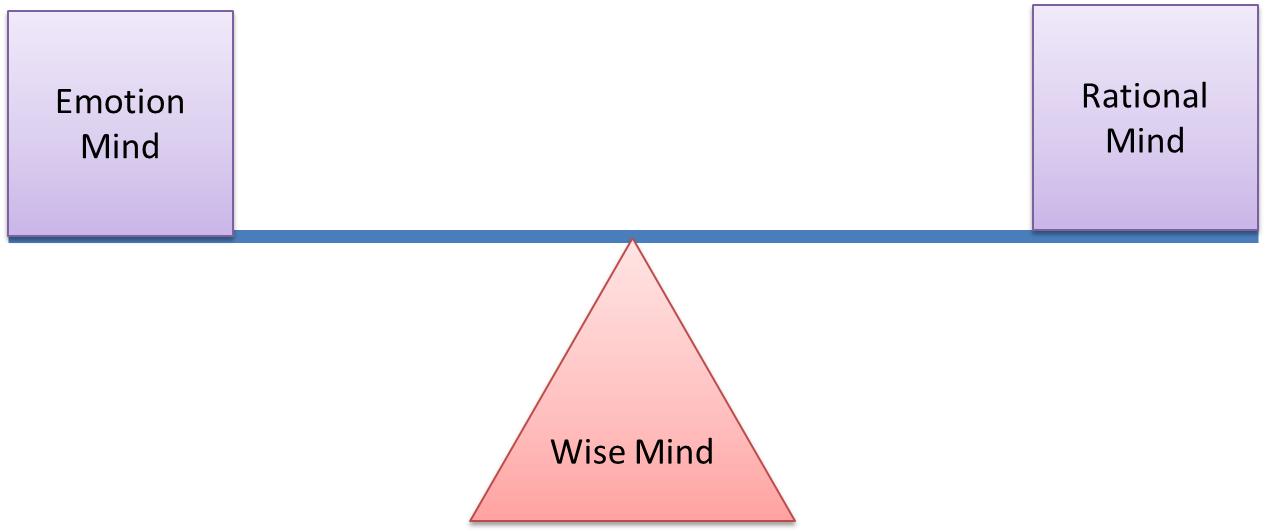
A dialectic, in the DBT sense, can be represented as a see-saw of extremes, with a healthy center-point. For instance, two state-of-mind extremes include Emotion Mind and Rational Mind. Emotion Mind is when a person’s thoughts and actions are governed entirely by emotions. This could be good – such as when someone is in love – but it is often bad. Too much emotion can lead to inappropriate decisions, behaviors, and unhealthy thoughts.
On the other side of the see-saw, a person might be in Rational Mind. Although this sounds good (and can be good when you are performing highly rational tasks like solving puzzles), it is generally not good to think exclusively in rational mind because you miss emotional components of the situation. For instance, a person who is entirely in rational mind is unable to experience empathy or react appropriately to emotional situations (this is often a complaint made about people with Asperger’s syndrome).
You are somewhere between rational and emotional mind at all times. The middle of the see-saw is called Wise Mind. Here, you can express the right amount of emotion and rational thought to make a clear-headed decision. DBT recognizes that people are often at the extremes of this see-saw, and asks that you use “skills” to move yourself back into Wise Mind before making decisions (such as breaking up with your significant other or self-harming).
Almost every situation has a dialectic see-saw. And according to DBT, it is often best to keep yourself in the middle of the two extremes. The middle would be a compromise. Of course, sometimes compromise is the wrong decision to make (such as when you need to cut ties with an abusive relationship), but compromise is generally best.
Skills that DBT suggest are separated into categories of mindfulness, interpersonal effectiveness, emotion regulation, and distress tolerance.
Mindfulness includes: grounding yourself in a situation, for instance, recognizing where you are, what you are doing, and what is going on around you; being nonjudgmental, for instance, one of my employees assumes that when the nurses say “she is awful to work with” that they are talking about her. This is a judgmental thought. To be non-judgmental, she would have to say “well, maybe they’re not talking about me. Why am I assuming they are?”
Interpersonal effectiveness entails balancing your own needs with the needs of others, building relationships, and being in Wise Mind when approaching difficult situations.
Emotion regulation includes being mindful of what emotions you’re feeling; being aware of what you want to do – for instance isolating – and doing the opposite; doing things that make you feel good – like leisure activities – or work that makes you feel accomplished – like writing a blog post; coping ahead, for instance, if I know that I will be upset tomorrow because it’s the anniversary of my mother’s death, I can plan some distracting activities to keep myself from brooding.
Distress tolerance includes distracting yourself when you feel upset; self-soothing by taking a bath or rubbing a smooth stone; and accepting reality.
Yes, all this mindfulness stuff might sound cheesy to a lot of you, but being aware of your emotions and how you’re reacting to them is an amazing way of changing the way you behave – and changing the way you behave can eventually remove your dysfunctional thoughts, as well.
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview



