

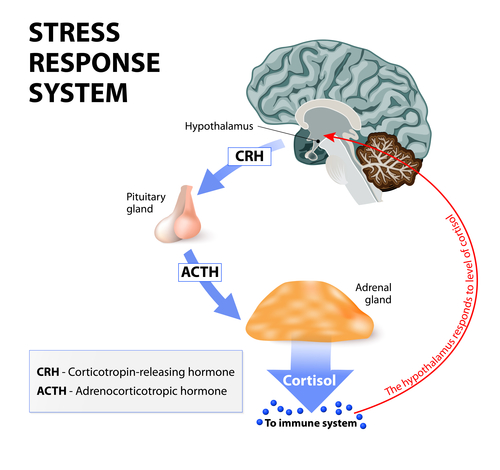
In order to understand why long-term stress can be bad, we need to understand what immediate effect stress has on our bodies. Under stress, the hypothalamus-pituitary-adrenal system (HPA axis) is activated. The hypothalamus releases corticotrophin-releasing-hormone (CRH). CRH stimulates the pituitary gland. The pituitary then secretes adrenocorticotrophic hormone (ACTH). The Adrenal cortex then produces the stress hormone cortisol in humans.
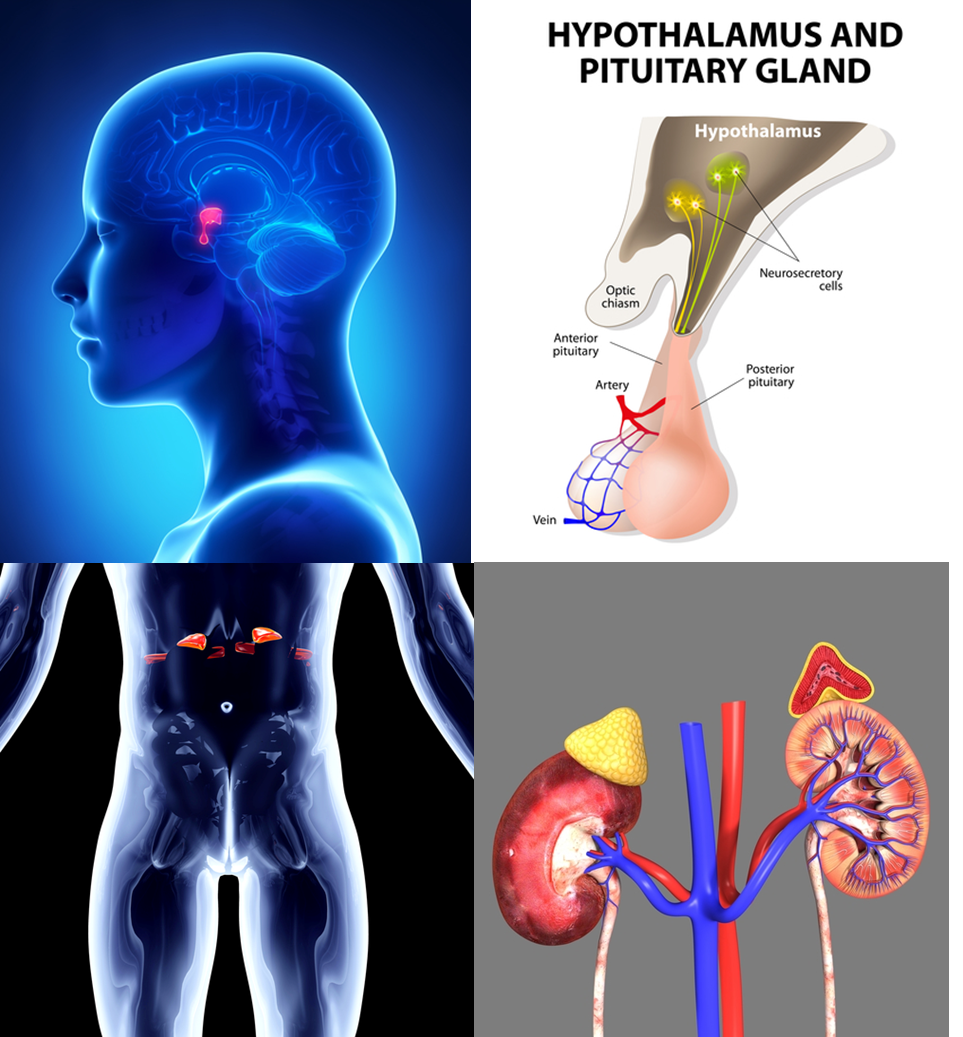 |
| Anatomy of hypothalamus-pituitary-adrenal system Top left, the pituitary gland is red Top right, the hypothalamus and pituitary glands are connected Bottom left, the adrenal glands are bright red Bottom right, the adrenal glands are the yellow cones on the kidneys |
Cortisol activates the fight-or-flight response. The sympathetic nervous system shuts down anything that your body doesn’t need during a traumatic event where you might need to fight or run away from a threat. That means your stomach stops digesting, you stop producing semen / ovulating, your immune system – which requires a huge amount of energy – slows way down. Tissue repair – also another drain on energy – halts. Activation of the sympathetic nervous system leads to release of the adrenaline (epinephrine) and noradrenaline (norepinephrine). These hormones circulate through the body and increase rate of the heart and of glucose metabolism – that gets the oxygen and energy flowing so you can use your limbs for fight or flight.
Cortisol is the hormone that prepares the body for fight-or-flight; thus, it is a good hormone to have around in an immediate danger. However, if stress continues, and cortisol is not turned off, the long term effects of suppression of vital bodily functions is quite detrimental to the body. Usually, after immediate stress, the cortisol has a feedback inhibition mechanism, in which it signals to slow its own production. However, if the stress continues for too long, cortisol’s feedback inhibition loop can be deactivated; thus allowing the adrenal cortex to continue pumping out cortisol and keeping the physiological effects of the sympathetic nervous system still active.
Since the immune system is inhibited by the sympathetic nervous system, individuals experiencing long-term stress are susceptible to infection by viruses and bacteria.
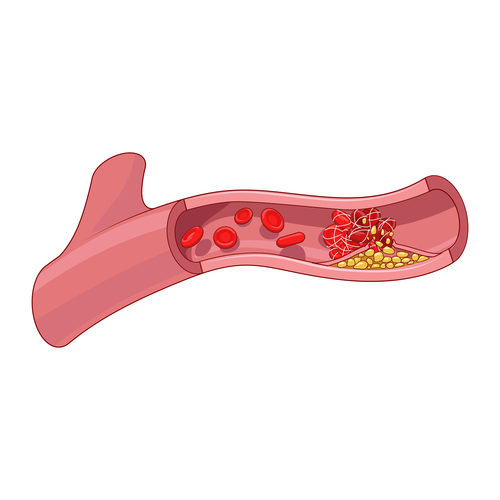
The best known physical side effect of stress is cardiovascular problems. As mentioned earlier in this post, the sympathetic nervous system increases heart-rate so that blood pumps more quickly throughout the body. Not only can this increase blood pressure directly, but it can also lead to damage of the blood vessel walls. The high blood pressure leads to tiny tears in the blood vessel walls. These tears are susceptible to accumulating circulating “junk” such as particles of fat and cholesterol. This accumulation – pictured n yellow above – can decrease blood flow through the vessel, or completely block flow as seen above. When the heart doesn’t get enough oxygen, then a heart attack may occur. Another problem with decreased blood flow is that if the brain doesn’t get enough oxygen, this can cause a stroke.
As you can see, stress can have a huge impact on your health. Doesn’t that stress you out?
This is a series of posts summarizing what I’m learning in my Abnormal Psychology course. Much of the information provided comes from reading my James N. Butcher’s textbook Abnormal Psychology. To read the other posts, follow these links:
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview
References:


