
Almost too late
we see the danger.
We could have been caught
drowned in the cesspool
because we couldn’t take the positive step
forward.
But the One friend calls.
Almost too late
we see the danger.
We could have been caught
drowned in the cesspool
because we couldn’t take the positive step
forward.
But the One friend calls.
This was a week of very little excitement. On Monday, we all went out for my nephew J’s birthday dinner (a little late because there had been snow delays the week before). Thursday I went out to a club with a friend – that was a bit of fun that I haven’t done for quite a while. And this weekend my nephew J has been staying with us. Friday night we discovered Galavant on Netflix. How funny! I’d never heard of it. Saturday we played a game of Fact or Crap (don’t ever play that game…boring) and then introduced J to Firefly. We unfortunately only got through the first few episodes before it was bedtime. Now he’ll have to wait a couple of weeks before he gets to see anymore.
Acquired
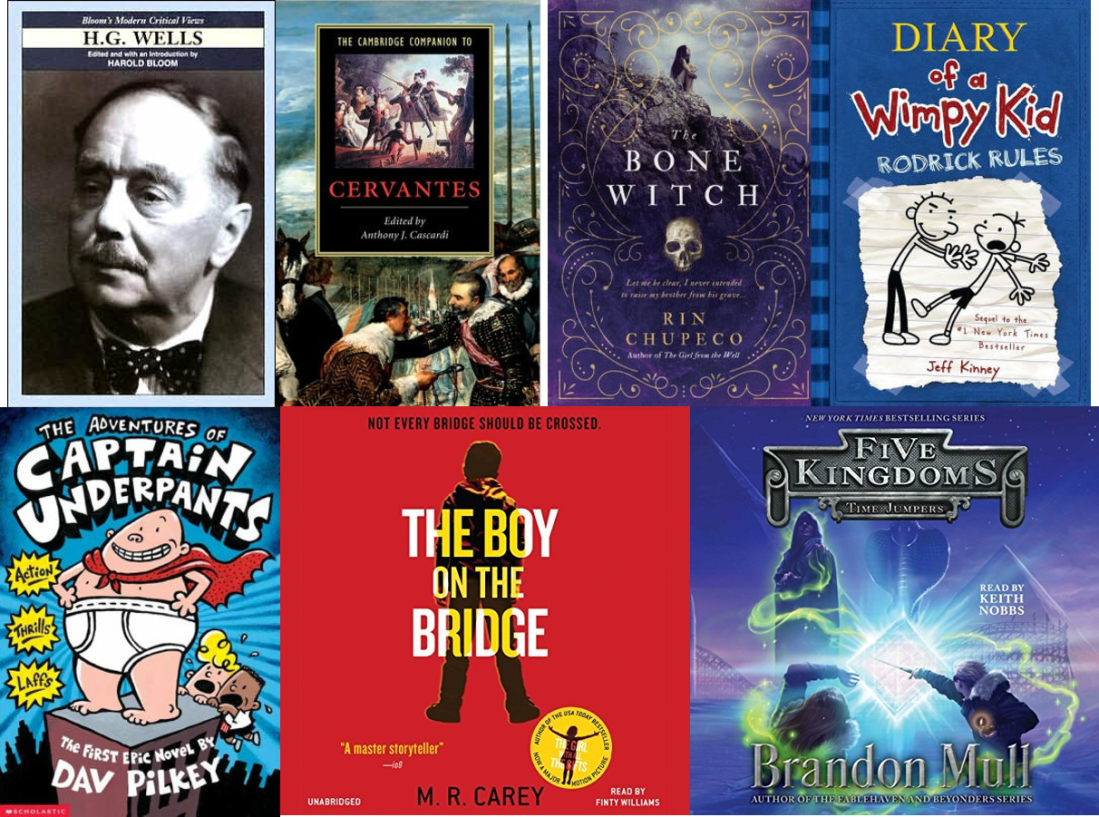
Since I’m studying Don Quixote, I went to Half-Price Books and acquired a copy of the Cambridge Companion to Cervantes, which I’ll read once I get through that gigantic novel on which I’m making very little progress. 🙂 And because I decided that I’ll break Don Quixote up with easier reading (H. G. Wells), I got a book of essays about Wells, edited by Harold Bloom. I was then at Barnes and Noble and feeling impulsive – so I bought The Bone Witch, which I think will be quite enjoyable light reading on my upcoming road trip. I used my Audible credits on The Boy on the Bridge and Time Jumpers. The former I will listen to as my real life book club choice for April. Time Jumpers is the fifth book in a series by my favorite middle grade author Brandon Mull. Finally, my dad bought copies of the second Diary of a Wimpy Kid book for D and The Adventures of Captain Underpants for M. Both were really excited about their new books, though I think M’s book was a bit too much over his reading level. He’s only 5. But dad didn’t want to get one kid a book and not get the other kid a book.
Completed
I did almost no reading. I got about half-way through this week’s Economist, and finished the last little bit of I Stop Somewhere.
Currently Reading
My hold for an H. G. Wells biography came up at the Library, so I set aside Don Quixote again and will work on H. G. Wells Desperately Mortal. Also moving back to Freeing Your Child from Anxiety. And I’m of-course listening to Brandon Mull’s new release. I really, really, really wish I could listen to audiobooks while driving on my upcoming road trip. J doesn’t mind the audiobooks, but they bore my dad silly. Maybe I’ll stick one earbud in my ear while I’m driving (which I’ll be doing ALL of). Or would that be ashamedly unsocial of me? I’m looking forward to being in Texas and maybe finding a walking path with NO SNOW ON IT. Wow. No snow. Just think. I love walking. Listening to an audiobook as I stroll along beside a lake….
On the blog
I published a few more stanzas of Facing My Demons 3, 4, 5, 6, 7, 8, & 9.
I published reviews of Island of Doctor Moreau, I Stop Somewhere, & Killers of the Flower Moon.
I published notes on the Coursera MOOC Solving the Opioid Crisis: A Physician’s Perspective, How Do Opioids Work, Analyzing Opioid Prescription Trends,
And I started participating in Top Ten Tuesday, because I liked the prompt.
Procrastination
As the cesspool rises to our chins
we panic.
Surely it will be worse further down.
We are paralyzed by indecision
all rational thought escapes.
Incongruously, I think:
Should I apply to that job tomorrow?
the one I think I won’t get?
Or do I buy a bottle of vodka
swim out into Lake Superior
as far as I can go?
To be washed out to sea
eaten by fish
escaping yet another rejection
another abandonment
another betrayal?
The final procrastination.

The University of Michigan is teaming up with Coursera to create Teach-Outs which are week-long MOOC lecture series which address problems currently faced in society today. Following will be notes for The Opioid Crisis.
 Jay S. Lee, MD, is a health services research fellow at the University of Michigan Center for Healthcare Outcomes & Policy, and a General Surgery resident at the University of Michigan. He received his undergraduate degree in Chemical Engineering from the University of Michigan, and his medical degree from the University of Michigan. Dr. Lee’s research focuses on characterizing variation in postoperative opioid prescribing and consumption, with a specific interest in opioid use after cancer surgery. His research is supported by a T32 training grant from the National Cancer Institute. After residency, he plans to complete a fellowship in Complex General Surgical Oncology, and pursue a career in academic surgery.
Jay S. Lee, MD, is a health services research fellow at the University of Michigan Center for Healthcare Outcomes & Policy, and a General Surgery resident at the University of Michigan. He received his undergraduate degree in Chemical Engineering from the University of Michigan, and his medical degree from the University of Michigan. Dr. Lee’s research focuses on characterizing variation in postoperative opioid prescribing and consumption, with a specific interest in opioid use after cancer surgery. His research is supported by a T32 training grant from the National Cancer Institute. After residency, he plans to complete a fellowship in Complex General Surgical Oncology, and pursue a career in academic surgery.
Cancer patients are generally given opioids post-surgery, and since the opioids help manage the patients’ pain, these prescriptions are a good use of opioids. However, these patients are often observed taking those medications longer than necessary. Years ago, doctors didn’t know how much opioid to prescribe, and often over-prescribed. Now that the epidemic is in the front of their minds, they are surveying patients to see how many opioids are actually being taken in order to make a guess at how much they should prescribe. They found the the actual number used is much lower than they have been prescribing. Doctors have also been spending more time talking to patients about the risks of opioid use, and patients have been responsive by taking less of the medication.
The discussion question that accompanied this lecture was: Several of our experts have mentioned the pharmaceutical industry’s aggressive promotion of opioids to doctors and patients as a significant contributing factor in the opioid crisis. Should there be some controls or limits on the pharmaceutical industry’s influence on physicians? If so, what should they be? If not, why?
Wow. Of course there should be some limits on the pharmaceutical industry’s influence on physicians! At the very least, physicians should receive no kickbacks from any pharmaceutical company, ever. I wish there could be a go-between who gathered all the information about the new meds and talked to the physicians in a disinterested way – rather than the physicians talking directly to people who are trying to market the drug.
Procrastination
It has stalked us through life
cementing us in imaginary complaisance.
We cannot do what we want to do:
the economy
selfish bosses
back-stabbing coworkers
bad advice
ill preparation
low chance of success
Excuses.
But they seem so real.
Only excuses.
But what is the real reason?
Those demons lie further down.
The University of Michigan is teaming up with Coursera to create Teach-Outs which are week-long MOOC lecture series which address problems currently faced in society today. The following are notes for lecture set 3 of Solving the Opioid Crisis.
 This lecture was given by Daniel Clauw, Professor of Anesthesiology, Medicine (Rheumatology) and Psychiatry at the University of Michigan. He serves as Director of the Chronic Pain and Fatigue Research Center. Until January 2009 he also served as the first Associate Dean for Clinical and Translational Research within the University of Michigan Medical School, and PI of the UM Clinical and Translational Sciences Award (CTSA).
This lecture was given by Daniel Clauw, Professor of Anesthesiology, Medicine (Rheumatology) and Psychiatry at the University of Michigan. He serves as Director of the Chronic Pain and Fatigue Research Center. Until January 2009 he also served as the first Associate Dean for Clinical and Translational Research within the University of Michigan Medical School, and PI of the UM Clinical and Translational Sciences Award (CTSA).
People are mainly focused on the deaths by overdose due to opioids, but another aspect of the epidemic is that many people are on opioids long term due to chronic pain. This is not a good use of opioids, since they do not target many forms of chronic pain, so doctors are no longer prescribing them (as often) for this purpose. Chronic pain that is located in a certain body part (such as in osteoarthritis) can be helped by a small dose of opioids, but pain originates in the nervous system (like fibromyalgia) is not helped by opioids.
Opioids bind the same receptors as endorphins, so when people are given opioids their endorphin systems are being hijacked. When someone has been on opioids for years, it is difficult to take them off because they no longer have a normally functioning endorphin system. There should be two sets of rules for prescribing opioids: those for people who have been on opioids chronically and those who are newly starting with a pain control regimen.
Until the 1990s, people who died of opioid overdose were heroine addicts that started on heroine. They were lower socioeconomic class, inner city, and black. Therefore, it wasn’t considered a major problem by the privileged classes. However, in the 90’s, doctors started over-prescribing opioids so that now, 60 to 70 percent of people who die of opioid overdose started with a prescription. That’s something the privileged majority is willing to pay attention to.
This lecture came with the following discussion question: Dan Clauw mentions the pharmaceutical industry’s argument that access to opioids are “a human right”. Do you agree with this sentiment? If so, why? If not, why?
I believe that healthcare and access to proper medications is a human right. However, I do not believe that there is a human right to be pain-free. If the risks of giving opioids outweighs the benefits, then opioids should not be prescribed.
Procrastination.
We would rather stand knee-deep
in sludge
frigid
Colder than is physically possible.
I should be numb
but I can feel disturbingly warm currents as well.
The levels rise.
The reek intensifies.
And yet we bicker.
Tears
Wall punching
Gut wrenching sobs
Cruel words that neither of us mean
Emotional destruction
is what we choose
rather than facing our demons inside.
 Summary: In the 1920s, the Osage Indians of Oklahoma were the richest people per capita due to the discovery of oil on their land. The federal government decided that the Osage were not “fit” to make monetary decisions on their own, and they were appointed legal guardians who did anything but guard the safety of their legal charges. Over a period of several years, many rich Osage were murdered (or died suspiciously) in what appears to be a conspiracy among legal guardians to gain control of the wealth. Outlining malicious greed and terror, Killers of the Flower Moon begins by following a specific set of murders that the FBI “solved.” Grann then continues the book by describing his own research into other mysterious deaths that happened around the same time.
Summary: In the 1920s, the Osage Indians of Oklahoma were the richest people per capita due to the discovery of oil on their land. The federal government decided that the Osage were not “fit” to make monetary decisions on their own, and they were appointed legal guardians who did anything but guard the safety of their legal charges. Over a period of several years, many rich Osage were murdered (or died suspiciously) in what appears to be a conspiracy among legal guardians to gain control of the wealth. Outlining malicious greed and terror, Killers of the Flower Moon begins by following a specific set of murders that the FBI “solved.” Grann then continues the book by describing his own research into other mysterious deaths that happened around the same time.
My Thoughts: This book is engaging and terrifying at the same time. It’s sadly too easy to believe that people appointed to be “guardians” would act so despicably. It is disgusting and bigoted that the federal government claimed the Osage needed guardians to begin with. Such a tragic story. But one that I think every American should read to understand how the government has treated Native Americans.

Procrastination.
This is the first demon two of us face.
Only the One friend
urges entry through the gate.
The other and I bicker
Bring up old angers that should have been buried
long ago.
So long ago.
The University of Michigan is teaming up with Coursera to create Teach-Outs which are week-long MOOC lecture series which address problems currently faced in society today. The following are notes for lecture set 2 of Solving the Opioid Crisis.
 This is an interview with Pooja Lagisetty, whose research interests focus on culturally tailored behavioral interventions, social determinants, health disparities, neighborhood determinants of chronic diseases, and urban design. She is a primary care physician who provides medication assisted therapy (MAT) for opioid addiction to patients at the Ann Arbor VA, has studied the literature about MAT in primary care, and is involved in efforts to increase the number of primary care teams that provide MAT to patients as a way to combat the shortage of treatment options.
This is an interview with Pooja Lagisetty, whose research interests focus on culturally tailored behavioral interventions, social determinants, health disparities, neighborhood determinants of chronic diseases, and urban design. She is a primary care physician who provides medication assisted therapy (MAT) for opioid addiction to patients at the Ann Arbor VA, has studied the literature about MAT in primary care, and is involved in efforts to increase the number of primary care teams that provide MAT to patients as a way to combat the shortage of treatment options.
In Dr. Lagisetty’s interview, she said that the opioid crisis is drawing international attention because people die of opioid overdose at much higher rates than of other drug types. However, it’s not just the overdosing that is a problem with opioids – there is a spectrum of severity, but that even people who will never overdose can have their lives hijacked by drug use.
Risk factors that doctors should look for are addiction to other drugs, lower socioeconomic status, depression/mental illness, misuse of drugs (higher or more frequent dosing than prescribed), and the use of the drug with benzodiazepines. (Though, personally, I am loathe to suggest doctors choose to not prescribe pain medications for people based on socioeconomic status or because they’re depressed!)
Medication assisted treatment of addiction (e.g. Methadone, Buprenorphine, Naltrexone) is more successful than quitting without medications, but there is very low accessibility. This low accessibility is due to many factors. For one, Methadone has to be prescribed within a specialized facility. Buprenorphine and Naltrexone can be taken home by patients, but must be prescribed by specialists. Unfortunately, there aren’t many specialists because there is a stigma attached to treating addiction patients, and many doctors don’t want to be associated with that stigma. Furthermore, there is a stigma for the patients that go to addiction specialists, so they are less likely to go than they would to a primary care physician.
Dr. Lagisetty suggests that the reason our society has such an opioid over-prescription problem in the US is because doctors treat pain like a vital sign: “how much pain are you in on a scale of 1 to 10?” Because of this understanding of pain as a vital sign, doctors and patients in the US now think that patients should be as pain-free as possible. She says that she doesn’t think other cultures are like that.
The first discussion question with this lecture was: As patients, should we ever experience pain? If so, when? If not, why?
Wow. I’m not sure how to answer that question. I can see where she’s going with the question – because of the addictive properties of opioids, where should doctors draw the line for prescribing pain medications? I simply don’t know the answer to that question. I’ve never been in real pain before, so I don’t want to make blanket statements about something I’ve never experienced. However, I have been around patients who have claimed to be in a lot of pain and were upset when the doctor didn’t prescribe them pain medications. At the time, I sympathized with them – though I recognized that the ones who complained the most about their pain were the ones who complained the most in general. And this is an example of where the squeaky wheel might not actually get the attention.
The second discussion question with this lecture was: How would you characterize your society’s attitude towards “acceptable pain,” and do you think it has changed over time? (Please indicate where you reside.)
I live in the US, and I’ve never thought about “acceptable pain.” Pain feels different to different people. We will never know how another person feels. Dr. Lagisetty says that in the US we think pain should be minimized if at all possible, and I suppose that’s probably true.
