Paraphilias are sexual behavior patterns in which unusual objects, rituals, or situations are required for full sexual satisfaction. And yes, believe it or not, paraphilic disorders are diagnosable in the DSM-5. But in order to have a disorder, you can’t just be turned on by unusual situations – it has to involve suffering or humiliation of yourself or others. (Though unfortunately, the suffering may be caused by stigma within society.) I will list several paraphilic disorders and discuss each:
Fetishistic Disorder: Individual has recurrent sexually arousing fantasies, urges, and behaviors involving inanimate objects (i.e. women’s underwear) or parts of the body (e.g. feet). People with fetishes are generally men.
Transvestic Disorder: Hetreosexual men who must be wearing women’s clothes in order to experience full sexual experience.
Voyeuristic Disorder: Individuals with voyeuristic disorder have intense sexual fantasies and behaviors of watching women undress or watching the sexual activities of others. People with this disorder are generally young men.
Exhibitionist Disorder: These individuals have intense sexual desire and behavior to sexually expose themselves to others. This generally is a man exposing himself to a young, unsuspecting woman; but sometimes they expose themselves to children.
My dad tells the story that one time he was standing in a check-outline for groceries, and a man laid it all out on the cashier’s countertop. Cool as a cucumber, and without even glancing at the man, she rang up a can of food and then whammed it down hard on…well, you know where. That man was hauled out in an ambulance. Sometimes bad decisions are made.
Frotteuristic Disorder: In frotteuristic disorder, someone is sexually excited by rubbing his genitals against an unwilling participant. I originally became familiar with this one due to a series of incidents (twice involving myself) with a coworker in retail. Very, very gross. Ick. But it was an experience to learn a new word when my dad was like “Oh! there’s a disorder for that!”
Sexual Sadism Disorder: The term “sadism” derives from the Marquis de Sade who got great sexual excitement out of inflicting cruelty upon people. Similarly, an individual with sadism disorder is aroused by psychologically or physically abusing someone. When sadism is inflicted upon a willing participant, it is not considered a disorder. But some sexual sadists inflict it upon partially or fully unwilling people.
Sexual Masochism Disorder: The term “masochism” is based on a fictional character created by Leopold V. Sacher-Masoch. In masochism disorder, an individual must get intense sexual pleasure from fantasizing about or indulging in the experience of pain.
Sado-masochistic relationships can be healthy and cooperative, within reason; however, masochism can lead to humiliating experiences and sometimes death.
This is a series of posts summarizing what I’m learning in my Abnormal Psychology course. Much of the information provided comes from reading my James N. Butcher’s textbook Abnormal Psychology. To read the other posts, follow these links:
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
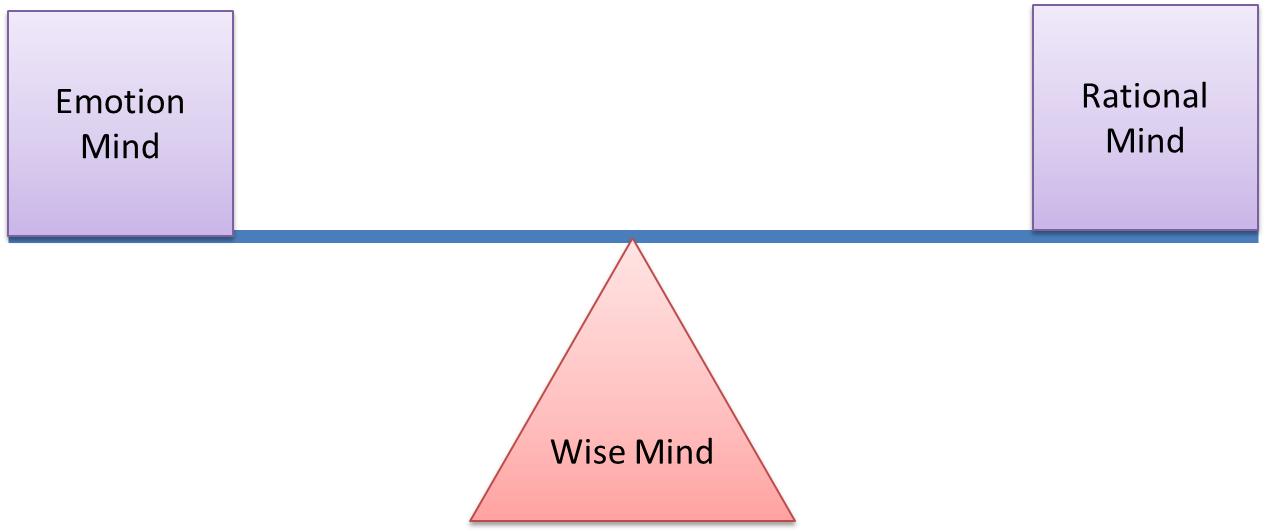
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview
Sexual Masochism Disorder: The term “masochism” is based on a fictional character created by Leopold V. Sacher-Masoch. In masochism disorder, an individual must get intense sexual pleasure from fantasizing about or indulging in the experience of pain.
Sado-masochistic relationships can be healthy and cooperative, within reason; however, masochism can lead to humiliating experiences and sometimes death.
This is a series of posts summarizing what I’m learning in my Abnormal Psychology course. Much of the information provided comes from reading my James N. Butcher’s textbook Abnormal Psychology. To read the other posts, follow these links:
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview
References:
Butcher, James N. Hooley, Jill M. Mineka, Susan. (2014) Chapter 12: Sexual Variance, Abuse, and Dysfunctions. Abnormal Psychology, sixteenth edition (pp. 405-442). Pearson Education Inc.