As mentioned in my opening post about personality disorders, personality disorders are split into three clusters: A, B, and C. This post will discuss the cluster A personality disorders. Cluster A disorders are characterized by distrust, suspiciousness, and social detachment. Often, people with cluster A personality disorders are considered eccentric or odd.
The characteristic traits of paranoid personality disorder are suspiciousness and mistrust of others, tendency to see oneself as blameless, and tendency to be on guard for perceived attacks by others. The disorder develops in early adulthood. To be diagnosed, a person must exhibit 4 or more of 7 traits: 1) he suspects, without sufficient basis, that others are exploiting, harming, or deceiving him; 2) he is preoccupied with unjustified doubts about the loyalty or trustworthiness of friends or associates; 3) he is reluctant to confide in others because of unwarranted fear that the information will be used maliciously against him; 4) he reads hidden demeaning or threatening meanings into benign remarks or events; 5) he persistently bears grudges; 6) he perceives attacks on his character or reputation that are not apparent to others and is quick to react angrily 7) he has recurrent suspicions, without justification, regarding fidelity of spouse or partner.
Of course, I am unqualified to diagnose anyone with a personality disorder, but I think real-life stories are helpful.
When I worked in retail, there was a guy that I had a crush on. We had been “friends” for almost a year, and I figured it was ok to tell him I liked him. He freaked out and said that I’d betrayed him (because he wasn’t ready to date anyone due to a bad experience in the past).
He soon became incredibly paranoid. He accused me to the manager first of stalking him within the store, then of calling his phone number just to hear the sound of his voice (mind you, this guy never handed his phone number out to anyone, so he was basically accusing me of sneaking into the office and illicitly looking up his number), and finally, he accused me of placing a kilo of marijuana near his car. (Though he couldn’t produce said kilo for evidence.)
Looking back, I realized his behavior had been odd all along. He was huge on conspiracy theory; stockpiled guns; thought everyone was out to get him; didn’t tell anyone where he lived, what his phone number was, or any personal details about his past; and he accused me of being nasty and demeaning when I made a casual comment “Oh, you’ve already started Christmas shopping? Seems a bit early.” And boy could he hold a grudge.
Since then, I’ve wondered what happened to this guy. He was really a sweet, caring person. I worry about his health and safety, since his paranoia clearly had a huge negative impact on his life.
This is one of the personality disorders that would be abolished if the next DSM adopts a dimensional approach as discussed in my previous post. I wonder what category these traits would fall into then?
Schizoid personality disorder is characterized by impaired social relationships and low desire to form attachments to others. To be diagnosed with schizoid personality disorder, a patient must have 4 of the following 7 traits: 1) he neither desires nor enjoys close relationships, including being part of a family; 2) he almost always chooses solitary activities; 3) he has little, if any, interest in having sexual experiences with another person; 4) he takes pleasure in few, if any, activities; 5) he lacks close friends or confidants other than first-degree relatives; 6) he appears indifferent to the praise or criticism of others; 7) he shows emotional coldness, detachment, or flattened affectivity.
This is another personality disorder that would disappear with the dimensional approach.
People with schizotypal personality disorder are also loners. People with scizotypal personality disorder tend to have superstitious beliefs, and some experience psychotic symptoms like believing they have magical powers. They can also be paranoid, have distorted speech, or see special meaning in ordinary objects or events. Schizotypal personality disorder is thought to be related to schizophrenia – perhaps a less severe manifestation or a precursor to schizophrenia.
In order to be diagnosed with schizotypal personality disorder, a patient must have five or more of the following traits: 1) he has ideas of reference (believing innocuous events or objects have strong personal meaning); 2) he almost always chooses solitary activities; 3) he has unusual perceptual experiences (mild hallucinations); 4) he has odd thinking and speech (e.g. vague, circumstantial, metaphorical, overelaborate, or stereotyped); 5) he exhibits suspiciousness or paranoid ideation; 6) he has inappropriate or constricted affect; 7) his behavior or appearance is odd or eccentric; 8) he has a lack of close friends or confidants other than first-degree relatives; 9) he has excessive social anxiety.
This is the only cluster A personality disorder that would not be lost if we switched to the dimensional approach of diagnosis.
This is a series of posts summarizing what I’m learning in my Abnormal Psychology course. Much of the information provided comes from reading my James N. Butcher’s textbook Abnormal Psychology. To read the other posts, follow these links:
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
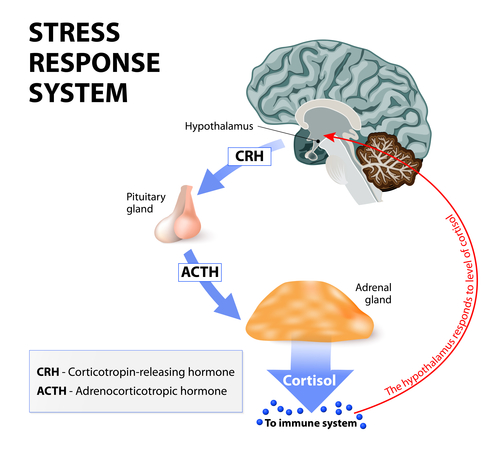
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview
This is another personality disorder that would disappear with the dimensional approach.
People with schizotypal personality disorder are also loners. People with scizotypal personality disorder tend to have superstitious beliefs, and some experience psychotic symptoms like believing they have magical powers. They can also be paranoid, have distorted speech, or see special meaning in ordinary objects or events. Schizotypal personality disorder is thought to be related to schizophrenia – perhaps a less severe manifestation or a precursor to schizophrenia.
In order to be diagnosed with schizotypal personality disorder, a patient must have five or more of the following traits: 1) he has ideas of reference (believing innocuous events or objects have strong personal meaning); 2) he almost always chooses solitary activities; 3) he has unusual perceptual experiences (mild hallucinations); 4) he has odd thinking and speech (e.g. vague, circumstantial, metaphorical, overelaborate, or stereotyped); 5) he exhibits suspiciousness or paranoid ideation; 6) he has inappropriate or constricted affect; 7) his behavior or appearance is odd or eccentric; 8) he has a lack of close friends or confidants other than first-degree relatives; 9) he has excessive social anxiety.
This is the only cluster A personality disorder that would not be lost if we switched to the dimensional approach of diagnosis.
This is a series of posts summarizing what I’m learning in my Abnormal Psychology course. Much of the information provided comes from reading my James N. Butcher’s textbook Abnormal Psychology. To read the other posts, follow these links:
The Definition of Abnormal
A History of Abnormal Psychology
Abnormal Psychology in Contemporary Society
Contemporary Viewpoints on Treating Mental Illness – Biology
Contemporary Viewpoints on Treating Mental Illness – Psychology
Frontline: New Asylums
Brave New Films: This is Crazy
Clinical Mental Health Diagnosis: Biological Assessment
Clinical Mental Health Diagnosis: Psychological Assessment
Does the DSM Encourage Overmedication?
Post Traumatic Stress Syndrome – The Basics
Panic Disorder
Obsessive Compulsive Disorder
Hoarding and Body Dysmorphic Disorders
Depression – an Overview
Personality Disorders – Clusters and Dimensions
Personality Disorders – Cluster A
Personality Disorders – Cluster B
Personality Disorders – Cluster C
Biological Effects of Stress on Your Body
Somatic Symptom and Related Disorders
Dissociative Disorders
Borderline Personality Disorder
Dialectical Behavioral Therapy
Paraphilic Disorders
Gender Dysphoria – Homosexuality and Transgender
Anxiety Disorders
Bipolar Disorder – The Basics
Suicide – An Overview
References:
Butcher, James N. Hooley, Jill M. Mineka, Susan. (2014) Chapter 10: Personality Disorders. Abnormal Psychology, sixteenth edition (pp. 328-366). Pearson Education Inc.